By a longitudinal section starting from the xyphoïde to the pubis, combined with an ascending bilateral section from the pubis to the antero superior iliac crest allowing a reclining of two greasy shred.
Figure 15 puts in evidence the given lustre aspect of the muscular aponeurosis. The section of the muscular wall is realized classically along the white line by protecting the anterior layer of the peritoneum.
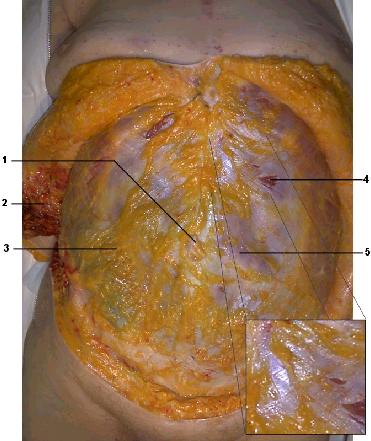
Figure 15 : Dissection of anterior wall
1 Median line ; umbilic
2 Sub cutaneous hematoma
3 Sub cutaneous fat attached to muscular aponeurosis
4 Accidental breach: External oblique muscle visible.
5 Aponeurosis
When muscular planes are reclined, we incise peritoneum to enter the peritoneal cavity (figure 16).
One can put in evidence on top-left the anterior wall of stomach, and transverse colon at its inferior edge.
Right and left colic angles, more posterior are not visible ; on the other hand, the inferior part of the right colon is visible.
On center, the greater omentum occupies the most part of the view. On top right, the inferior edge of the liver is visible.
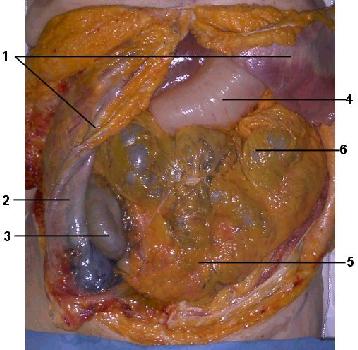
Figure 16 : Anterior view of peritoneal cavity after wall resection.
1 Reclined muscles
2 Posterior layer of muscular wall with reclined parietal posterior peritoneum.
3 Right colon
4 Stomach
5 Grand omentum
6 Transverse colon
If one lifts the anterior wall; the falciform ligament of the liver is individualizable. (Figure 17)

Figure 17 : Falciform ligament of liver. View from below.
1 Liver suspensor ligament
2 Liver
3 Stomach
4 Greater omentum
Then, we resect the greater omentum to reach the intestinal loops.